
Have you done this too? The pain starts, the lights go off, a pill goes in, and you tell yourself one nap will fix it. Migraine is usually less polite than that. It is more like an alarm system set far too sensitive: a little smoke appears, and the whole building starts screaming.
Lead: Migraine is not a character test. Using Taiwan prevalence data, medication-overuse guidance, CGRP-targeted therapy reviews, the 2024 American Headache Society update, and a BMJ dietary trial, this article asks three practical questions: how do you know it is not “just a headache,” why can painkillers start working against you, and what exactly is new about the CGRP era?
Migraine is not defined by one-sided pain
The real issue in migraine is not left versus right. It is a pain network in the brain that becomes too ready to fire.
A population survey from Taipei estimated migraine prevalence at 9.1% in people aged 15 years and older, with 14.4% in women and 4.5% in men. Only 18% of those participants reported having previously received a formal diagnosis of migraine. That gap matters.
The name itself can mislead people. Migraine does not always stay on one side, and it does not always look dramatic in the same way. Some people feel a band-like squeeze. Some feel a pulse hammering in the temple. Some get worse the moment they move, along with nausea, light sensitivity, or sound sensitivity. When that happens, ordinary sensory input starts getting amplified by a pain pathway that is already turned up too high.
If your headaches keep coming back and are tied to nausea, photophobia, or worsening with activity, do not dismiss them as simple fatigue. Write them down. Pattern matters.
Why painkillers can start fighting you
Acute pain medicine matters, but when it becomes too frequent, control can flip in the wrong direction.
Many people reach for medication as soon as the pain starts. That is not automatically a problem. The problem starts when rescue medication becomes a long-term living arrangement. A 2022 guideline on medication-overuse headache warns that frequent acute treatment should raise concern, especially when triptans, opioids, or combination analgesics exceed 10 days per month, or when simple analgesics exceed 15 days per month.
Why does this happen? For some patients, the brain’s pain-control system behaves like an overworked call center: first it keeps taking every call, then it burns out. The medicine that once put out fires can become part of the background condition that keeps the alarm ringing.
This does not mean acute medicine should never be used. It means timing and frequency both matter. If attacks are getting more frequent and your month is being organized around rescue tablets, it is time to discuss prevention instead of only escalating self-treatment.
Why CGRP became a turning point
The key shift with CGRP-targeted therapy is not simply stronger treatment. It is treatment aimed directly at a core migraine pain pathway.
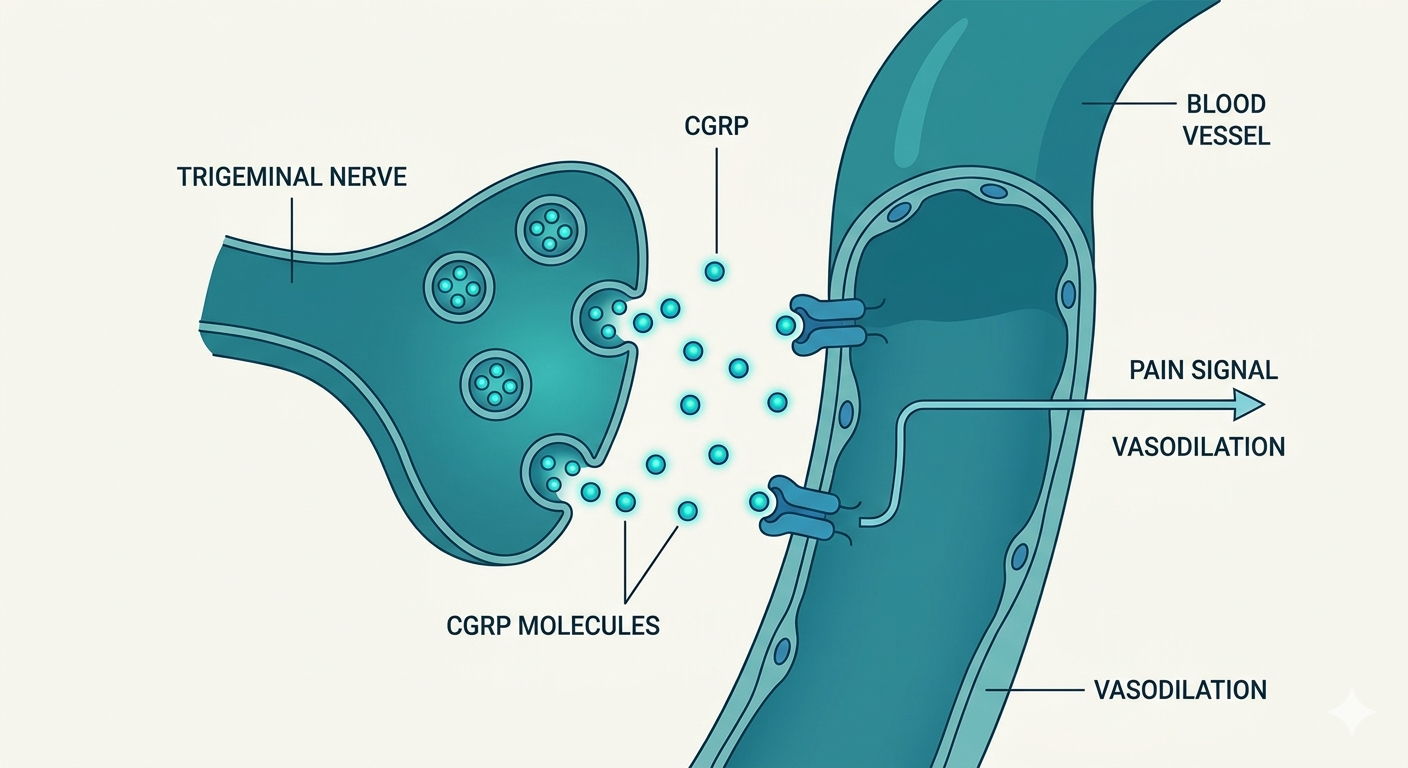
CGRP, or calcitonin gene-related peptide, is deeply involved in trigeminal pain signaling. During migraine attacks, that system helps amplify pain, vascular responses, and neurogenic inflammation. A 2018 review in Nature Reviews Neurology described CGRP-related treatment as the first wave of therapies designed specifically for migraine rather than borrowed from other diseases.
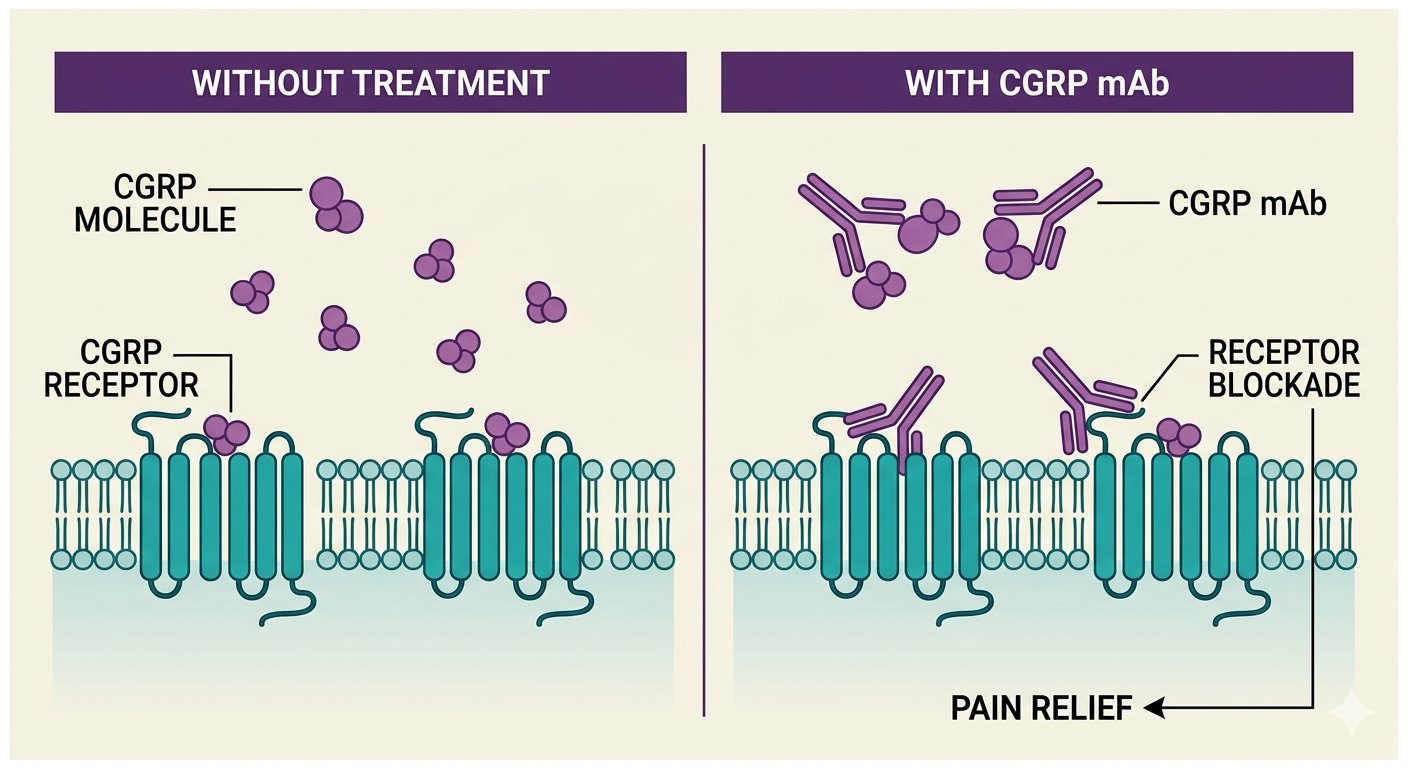
That is why many clinicians see a true treatment shift here. Older preventive options such as blood pressure drugs, antiseizure drugs, or antidepressants can help, but they were never built for migraine itself and some patients stop because of adverse effects. In 2024, the American Headache Society updated its position statement and listed CGRP-targeting therapies as a first-line option for migraine prevention.
Still, first-line does not mean universal. Cost, access, pregnancy planning, comorbidities, and attack frequency all change the decision. Long-term individualized outcomes also still need ongoing study. New tools matter, but they are not magic.
Does food matter
Diet can influence migraine, but it is better understood as tuning than as a single villain.
A 2021 randomized trial in BMJ found that increasing Omega-3 while lowering Omega-6 improved headache burden in adults with migraine. That matters because it suggests the dinner plate can interact with the same inflammatory and pain biology involved in migraine.
But it is a mistake to assume one food explains everything. Chocolate, cheese, coffee, or alcohol may trigger some people and not others. More common problems are skipped meals, dehydration, sleep disruption, and major schedule shifts. The migraine brain usually likes stability.
The most practical tool is still a headache diary. If you track attack time, sleep, meals, menstrual timing, stress, food, and medication, you give yourself and your clinician a real map instead of guesses.
What you can do now
If headache is already organizing your calendar, the sooner you map it, the better your chances of taking control back.
Look at three things first: how often attacks happen, how often acute medicine is needed, and whether headache is now affecting work, sleep, parenting, or relationships. If the answer keeps moving toward yes, stop treating it as something you simply have to endure.
Useful first steps are plain and boring, which is exactly why they work: stabilize wake time, avoid long fasting gaps, hydrate, build up aerobic activity gradually, and keep a clear diary. If a physician thinks preventive treatment is needed, CGRP-targeted options, traditional preventive drugs, and lifestyle changes often work best as a sequence rather than as competitors.
Migraine is not only pain in the head. It is more like a household smoke alarm set too sharp. Even a small signal makes it scream. The good news is that systems like this can be adjusted. The first step is to stop treating migraine as a problem that should simply be tolerated.
Found this useful?
Follow for new AI × biomedical research notes:
Or buy me a coffee to keep new content coming.
☕ Buy Me a Coffee